")







 Injectable weight loss drugs can improve heart health. Depositphotos –
Injectable weight loss drugs can improve heart health. Depositphotos –
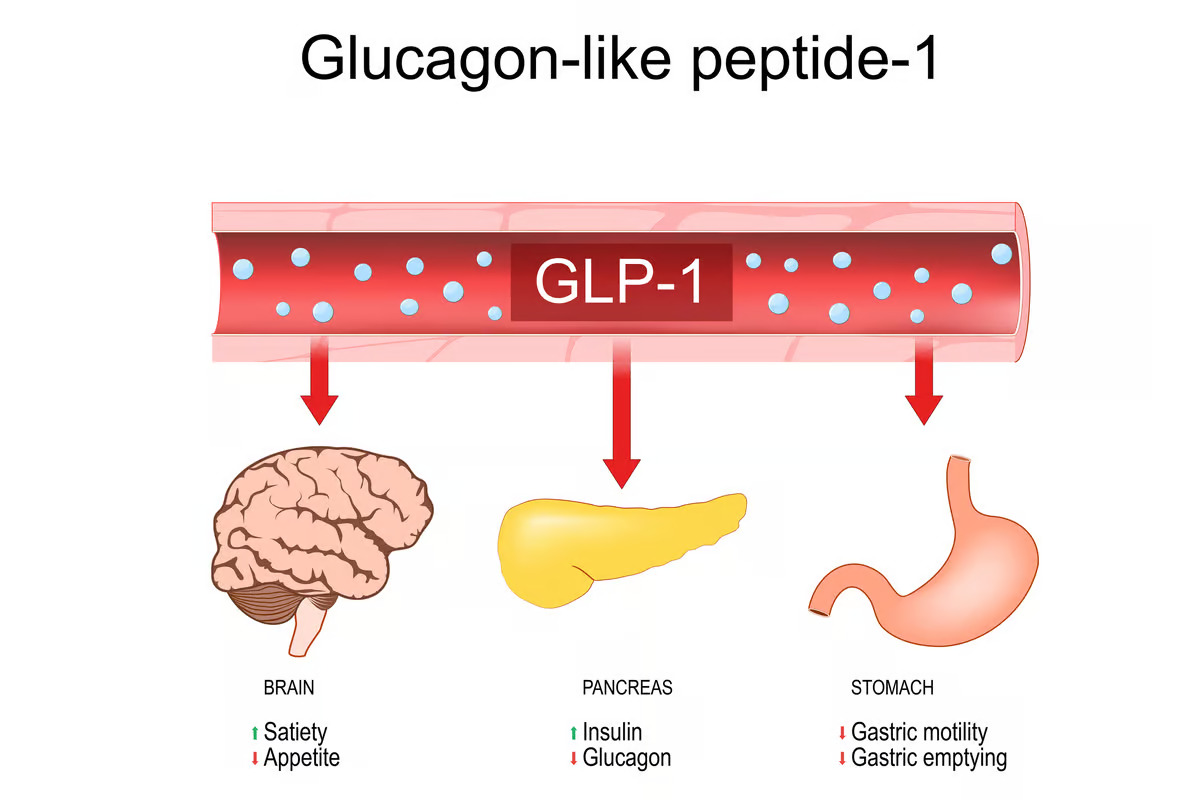
You might be sick of hearing about glucagon-like peptide-1 receptor agonists or GLP-1RAs, but this class of drugs keeps revealing its potential to revolutionize medicine beyond weight loss and diabetes treatment. Three studies presented at the AHA Scientific Sessions 2024, two of which concerned the use of GLP-1RAs, have added to the growing evidence of how these drugs are good for heart health.
“These studies reinforce the potential of GLP-1-based therapies not only to aid in weight loss but also to transform cardiac health, offering hope for patients living with obesity and cardiovascular disease,” said Harlan Krumholz, MD, editor-in-chief of the Journal of the American College of Cardiology (JACC), in which the studies were published. “As the science evolves, we are achieving a deeper understanding of how weight loss, and treatment with these medications, can improve outcomes across diverse patient populations with obesity.”
Obesity increases cardiovascular morbidity and mortality due to its direct and indirect effects. Directly, adipokines secreted by adipose (fatty) tissue contribute to an obesity-related low-grade inflammation or the development of metabolic syndrome, a constellation of diseases including type 2 diabetes, heart (cardiovascular) disease and the accumulation of plaques on artery walls or atherosclerosis. Indirectly, obesity accelerates the process of atherosclerosis and heart failure because of its impact on blood pressure, blood cholesterol levels, type 2 diabetes, and obstructive sleep apnea.
Following bypass surgery, semaglutide improved cardiac outcomes
The Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT) trial was a randomized, placebo-controlled trial that enrolled 17,604 patients over 45 with pre-existing cardiovascular disease and obesity but not diabetes. Patients received either once-weekly injections of 2.4 mg of the GLP-1RA semaglutide or a placebo. The data showed that those who received semaglutide had a reduced incidence of death from cardiovascular causes after almost 40 months.
For the present study, the researchers conducted a secondary analysis of the SELECT data, focusing on overweight or obese patients who previously had coronary artery bypass graft (CABG) surgery to correct a blockage or narrowing in one or more of the heart’s arteries. In the analysis, 2,057 participants had a history of CABG, and the majority (15,547) didn’t. The participants who’d had CABG surgery were older, largely (84%) male, and had a lower body mass index or BMI.

The researchers observed that semaglutide led to a consistent reduction in major adverse cardiovascular events (MACE) in the CABG and non-CABG groups, but the absolute risk reduction of MACE was greater in those who’d had bypass graft surgery: 2.3% vs. 1%. In this study, MACE included non-fatal stroke, non-fatal heart attack, hospitalization for heart failure, death from a heart-related cause and all-cause death. The magnitude of the benefit of semaglutide on the incidence of non-fatal heart attacks was higher in those with a history of CABG compared to those without. Also, as a positive ‘side benefit,’ semaglutide was also noted to reduce the incidence of diabetes in the group who’d had CABG surgery.
Tirzepatide alters heart structure and decreases risk of heart failure
Tirzepatide is a newer obesity/diabetes treatment that, unlike semaglutide, is a dual receptor agonist. Like semaglutide, it binds to GLP-1 receptors, mimicking the actions of the GLP-1 hormone to enhance insulin secretion and suppress appetite. But it also targets glucose-dependent insulinotropic polypeptide (GIP) receptors to stimulate the pancreas to release insulin.
Obesity increases the risk of developing a form of heart failure called ‘heart failure with preserved ejection fraction.’ Abbreviated to HFpEF, it’s generally pronounced heff-peff. The left ventricular ejection fraction (LVEF) is the volume of blood pumped out of the heart’s lower left chamber or ventricle, to the body. Patients with HFpEF present with the clinical features of heart failure – for example, shortness of breath, fatigue and weakness, and swelling in the lower extremities – but with normal or near-normal (hence, preserved) EF. It’s common in heart failure for the left ventricle (LV) to become enlarged or hypertrophied.
The original SUMMIT trial demonstrated that the dual receptor effect of tirzepatide led to significant weight loss and a decrease in death and worsening heart failure events in obesity-related HFpEF. Like the aforementioned semaglutide study, the researchers did a deeper dive into the parent study. They examined SUMMIT data to determine the effects of tirzepatide on heart structure and function, with the underlying hypothesis that the drug would decrease LV mass and fat deposits on the surface of the heart (epicardial adipose tissue, EAT).
In the video below, Baylor University Medical Center cardiologist Milton Packer, MD, the lead author of the present study, discusses the results following his presentation at the American Heart Association (AHA) Scientific Sessions 2024 in Chicago.
–
The researchers found that their hypothesis was correct. In patients treated with tirzepatide, LV mass decreased by 11 g (0.4 oz), and cardiac adipose tissue dropped by 45 mL (1.5 fl oz). They concluded that these reductions may have contributed to the reduction in heart failure events seen in the SUMMIT trial.
Lifestyle interventions like exercise affect biomarkers of heart function
The third study published in JACC is not concerned with GLP-1RAs but is another secondary analysis of a parent study and concerns heart health as it relates to weight loss via lifestyle interventions. So, it fits in nicely alongside the other two studies.
The LookAHEAD trial was a randomized controlled trial comparing the effect of an intensive lifestyle intervention – diet and exercise – to a diabetes support and education intervention on cardiovascular disease in overweight and obese type 2 diabetics. The cardiovascular disease event rate was very low in both groups, but there was no difference in cardiovascular outcomes between the groups. Although the intensive lifestyle intervention did not outshine the support and education intervention as it was expected to, participants exposed to the lifestyle intervention did show a large number of improvements in biomarkers of glucose and lipid control, less sleep apnea, less depression, improved insulin sensitivity and reduced need of diabetes medications.

In their substudy of the LookAHEAD trial, the researchers examined the effect of each intervention on two specific cardiac biomarkers, NT-proBNP and hs-cTnT, both of which are associated with cardiovascular outcomes. N-terminal pro-B-type natriuretic peptide (NT-proBNP) levels go up and down depending on whether heart failure is worsening or improving. High-sensitivity cardiac troponin T (hs-cTnT) is useful for evaluating damage to the cardiac muscle, even when it’s present in very small amounts.
Analyzing the trial data, the researchers found that in adults with type 2 diabetes, an intensive lifestyle intervention targeting weight loss led to a sustained reduction in hs-cTnT but a short-lived increase in NT-proBNP levels that fell over time. They concluded that the longitudinal assessment of both biomarkers provided information about a patient’s risk of atherosclerosis, but only changes in NT-proBNP predicted the risk of heart failure.
All three studies were published in the Journal of the American College of Cardiology: the semaglutide study here, the tirzepatide study here, and the lifestyle intervention study here. They were also presented at the American Heart Association’s (AHA) Scientific Sessions 2024 in Chicago.
Sources: American College of Cardiology, American Heart Association
Tags